




 Views Today : 95
Views Today : 95
Swimmer’s itch
| Swimmer’s itch | |
|---|---|
 |
|
| Cercarial dermatitis on lower legs, four days after spending a day in the shallows of a lake | |
| Specialty | Infectious disease |
Swimmer’s itch or cercarial dermatitis, is a short-term allergic immune reaction occurring in the skin of humans that have been infected by water-borne schistosomes. Symptoms, which include itchy, raised papules, commonly occur within 1–2 days of infection and do not generally last more than 2–3 weeks. However, people repeatedly exposed to cercariae develop heavier symptoms with faster onset.[1] Cercarial dermatitis is common in freshwater, brackish and marine habitats worldwide.[2] Incidence may be on the rise, although this may also be attributed to better monitoring. Nevertheless, the condition has been regarded as emerging infectious disease.[3]
There are no permanent effects to people from this condition.[4] Orally administered hydroxyzine, an antihistamine, is sometimes prescribed to treat swimmer’s itch and similar dermal allergic reactions. In addition, bathing in oatmeal, baking soda, or Epsom salts can also provide relief of symptoms.[5]
Cause[edit]
Swimmer’s itch probably has been around as long as humans. The condition was known to exist as early as the 1800s, but it was not until 1928 that a biologist found that the dermatitis was caused by the larval stage of a group of flatworm parasites in the family Schistosomatidae.[6] The genera most commonly associated with swimmer’s itch in humans are Trichobilharzia[1] and Gigantobilharzia. It can also be caused by schistosome parasites of non-avian vertebrates, such as Schistosomatium douthitti, which infects snails and rodents. Other taxa reported to cause the reaction include Bilharziella polonica and Schistosoma bovis. In marine habitats, especially along the coasts, swimmer’s itch can occur as well.[7]
These parasites use both freshwater snails and vertebrates as hosts in their parasitic life cycles as follows:
- Once a schistosome egg is immersed in water, a short-lived, non-feeding, free-living stage known as the miracidium emerges. The miracidium uses cilia to follow chemical and physical cues thought to increase its chances of finding the first intermediate host in its life cycle, a freshwater snail.
- After infecting a snail, it develops into a mother sporocyst, which in turn undergoes asexual reproduction, yielding large numbers of daughter sporocysts, which asexually produce another short-lived, free-living stage, the cercaria.
- Cercariae use a tail-like appendage (often forked in genera causing swimmer’s itch) to swim to the surface of the water; and use various physical and chemical cues in order to locate the next and final (definitive) host in the life cycle, a bird. These larvae can accidentally come into contact with the skin of a swimmer. The cercaria penetrates the skin and dies in the skin immediately. The cercariae cannot infect humans, but they cause an inflammatory immune reaction. This reaction causes initially mildly itchy spots on the skin. Within hours, these spots become raised papules which are intensely itchy. Each papule corresponds to the penetration site of a single parasite.
- After locating a bird, the parasite penetrates through the skin (usually the feet), dropping the forked tail in the process. Inside the circulatory system, the immature worms (schistosomula) develop into mature male and female worms, mate and migrate through the host’s circulatory system (or nervous system in case of T. regenti) to the final location (veins feeding the gastrointestinal tract) within the host body. There they lay eggs in the small veins in the intestinal mucosa from which they make their way into the lumen of the gut, and are dumped into the water when the bird defecates. One European species, Trichobilharzia regenti, instead infects the bird host’s nasal tissues and larvae hatch from the eggs directly in the tissue during drinking/feeding of the infected birds.[8]

Risk factors[edit]

Humans usually become infected after swimming in lakes or other bodies of slow-moving fresh water. Some laboratory evidence indicates snails shed cercariae most intensely in the morning and on sunny days, and exposure to water in these conditions may therefore increase risk. Duration of swimming is positively correlated with increased risk of infection in Europe[9] and North America,[10] and shallow inshore waters may harbour higher densities of cercariae than open waters offshore. Onshore winds are thought to cause cercariae to accumulate along shorelines.[11] Studies of infested lakes and outbreaks in Europe and North America have found cases where infection risk appears to be evenly distributed around the margins of water bodies[9] as well as instances where risk increases in endemic swimmer’s itch “hotspots”.[11] Children may become infected more frequently and more intensely than adults but this probably reflects their tendency to swim for longer periods inshore, where cercariae also concentrate.[12] Stimuli for cercarial penetration into host skin include unsaturated fatty acids, such as linoleic and linolenic acids. These substances occur naturally in human skin and are found in sun lotions and creams based on plant oils.
Control[edit]

Various strategies targeting the mollusc and avian hosts of schistosomes, have been used by lakeside residents in recreational areas of North America to deal with outbreaks of swimmer’s itch. In Michigan, for decades, authorities used copper sulfate as a molluscicide to reduce snail host populations and thereby the incidence of swimmer’s itch. The results with this agent have been inconclusive, possibly because:
- Snails become tolerant
- Local water chemistry reduces the molluscicide’s efficacy
- Local currents diffuse it
- Adjacent snail populations repopulate a treated area[13]
More importantly, perhaps, copper sulfate is toxic to more than just molluscs, and the effects of its use on aquatic ecosystems are not well understood.
Another method targeting the snail host, mechanical disturbance of snail habitat, has been also tried in some areas of North America[11] and Lake Annecy in France, with promising results. Some work in Michigan suggests that administering praziquantel to hatchling waterfowl can reduce local swimmer’s itch rates in humans.[14] Work on schistosomiasis showed that water-resistant topical applications of the common insect repellent DEET prevented schistosomes from penetrating the skin of mice.[15] Public education of risk factors, a good alternative to the aforementioned interventionist strategies, can also reduce human exposure to cercariae.
See also[edit]
References[edit]
- ^ Jump up to:a b Macháček, Tomáš; Turjanicová, Libuše; Bulantová, Jana; Hrdý, Jiří; Horák, Petr; Mikeš, Libor (2018-10-09). “Cercarial dermatitis: a systematic follow-up study of human cases with implications for diagnostics”. Parasitology Research. 117 (12): 3881–3895. doi:10.1007/s00436-018-6095-0. ISSN 0932-0113. PMID 30302587.
- ^ “Avian Schistosome Biodiversity”. www.schistosomes.net. Retrieved 2016-03-07.
- ^ Horák, Petr; Mikeš, Libor; Lichtenbergová, Lucie; Skála, Vladimír; Soldánová, Miroslava; Brant, Sara Vanessa (January 2015). “Avian schistosomes and outbreaks of cercarial dermatitis”. Clinical Microbiology Reviews. 28 (1): 165–190. doi:10.1128/CMR.00043-14. ISSN 1098-6618. PMC 4284296. PMID 25567226.
- ^ “With warm weather, Swimmers Itch makes annual appearance”. dnr.wi.gov. Retrieved 2016-03-07.
- ^ In CDC. “Swimmers Itch FAQS.” retrieved May 12, 2014
- ^ “Swimmer’s Itch in Michigan” (PDF). State of Michigan. 2014. Retrieved 5 March 2015.
- ^ Brant S, Cohen A, James D, Hui L, Hom A, Loker E (2010). “Cercarial Dermatitis Transmitted by Exotic Marine Snail”. Emerging Infectious Diseases. 16 (9): 1357–65. doi:10.3201/eid1609.091664. PMC 3294964. PMID 20735918.
- ^ Horák P., Kolářová L., Dvořák J. (1998). “Trichobilharzia regenti n. sp. (Schistosomatidae, Bilharziellinae), a new nasal schistosome from Europe”(PDF). Parasite. 5 (4): 349–357. doi:10.1051/parasite/1998054349. PMID 9879557.
- ^ Jump up to:a b Chamot E, Toscani L, Rougemont A (1998). “Public health importance and risk factors for cercarial dermatitis associated with swimming in Lake Leman at Geneva, Switzerland”. Epidemiol. Infect. 120 (3): 305–14. doi:10.1017/S0950268898008826. PMC 2809408. PMID 9692609.
- ^ Lindblade KA (1998). “The epidemiology of cercarial dermatitis and its association with limnological characteristics of a northern Michigan lake”. J. Parasitol. 84 (1): 19–23. doi:10.2307/3284521. JSTOR 3284521. PMID 9488332.
- ^ Jump up to:a b c Leighton BJ, Zervos S, Webster JM (2000). “Ecological factors in schistosome transmission, and an environmentally benign method for controlling snails in a recreational lake with a record of schistosome dermatitis”. Parasitol. Int. 49 (1): 9–17. doi:10.1016/S1383-5769(99)00034-3. PMID 10729712.
- ^ Verbrugge LM, Rainey JJ, Reimink RL, Blankespoor HD (2004). “Prospective study of swimmer’s itch incidence and severity”. J. Parasitol. 90(4): 697–704. doi:10.1645/GE-237R. PMID 15357056.
- ^ Blankespoor, H. D., Reimink, R. L. (1991). “The control of swimmer’s itch in Michigan: Past, present, and future”. Michigan Academician. 24 (1): 7–23.
- ^ Blankespoor, C. L., Reimink, R. L., Blankespoort, H. D. (2001). “Efficacy of praziquantel in treating natural schistosome infections in common mergansers”. Journal of Parasitology. 87 (2): 424–6. doi:10.1645/0022-3395(2001)087[0424:EOPITN]2.0.CO;2. PMID 11318576.
- ^ Salafsky, B., Ramaswamy, K., He, Y. X., Li, J., Shibuya, T. (November 1999). “Development and evaluation of LIPODEET, a new long-acting formulation of N, N-diethyl-m-toluamide (DEET) for the prevention of schistosomiasis”. Am. J. Trop. Med. Hyg. 61 (5): 743–50. PMID 10586906.
External links[edit]
| Classification |
|---|
| Wikimedia Commons has media related to Schistosome cercarial dermatitis. |
Malignes Melanom:
https://www.patologi.com/malignes%20melanom%202015.pdf
Sykdom. Vitenskap, kultur eller begrep for sårbarhet, håp, mestring og mot? PDF.
Sykdom.
Bjørn Hofmann, Høyskolen i Gjøvik. Universitetet i Oslo. https://patologi.com/wordpress/wp-content/uploads/2020/02/sykdomvitenskap.pdf
“Filleristing”/ Shaken-baby-syndrome Svenske rettsmedisinere har nok også bakgrunn/ utdannelse som patologer, og kan således vurdere bedre bl.a. funn ved rettsmedisinsk undersøkelse, i forhold til mulig legemlige sykdommer, altså ikke rettsmedisinsk årsak. Dette gjelder også nærmest alle rettsmedisinere i Norge, utenom noen kjente rettsmedisinere i Oslo, som mangler denne bakgrunnen. Fra NRK: https://www.nrk.no/osloogviken/xl/strid-om-diagnosen-filleristing_-ogsa-kalt-shaken-baby-syndrome-1.14849820
Foreldre dømmes til fengsel. Barn blir tatt fra foreldre. Familier går i oppløsning. Diagnosen «filleristing» er en rettsskandale | Wester og Eriksson Svenske og norske rettsmedisinere har totalt forskjellig syn på beviskraften.
Tatt fra: KRONIKK AFTENPOSTEN, 3.5.2019.
Knut Wester professor emeritus i nevrokirurgi, Universitetet i Bergen. Anders Eriksson seniorprofessor i rettsmedisin, Umeå Universitet
Sveriges Radio P3 har laget en rystende podkast kalt «Shaken baby-skandalen». Der forteller de om to familier som fikk livet ødelagt fordi deres spebarn ble feildiagnostisert som filleristet.
Foreldre ble fengslet i årevis, barn ble fjernet fra hjemmet og plassert i fosterhjem, dels på permanent basis, og det tok mange år før dommene ble opphevet av svensk høyesterett.
Det samme skjer i Norge. Vi har opplevd tilsvarende historier flere ganger etter at vi i relativt høy alder ble involvert i slike saker.
Knut Wester er professor emeritus i nevrokirurgi ved Universitetet i Bergen. Anders Eriksson er seniorprofessor i rettsmedisin ved Umeå Universitet.
Teori basert på to babyer
Vi var begge tidligere av den oppfatning at diagnosen filleristing (engelsk «shaken baby syndrome» eller«abusive head trauma») var basert på sikker vitenskapelig dokumentasjon, så solid at den ikke kunne trekkes i tvil. Denne dokumentasjonen tillegges av rettsmedisinere avgjørende vekt i norske rettssaker og har svært alvorlige konsekvenser for foreldre og familier.
En nøyaktig gjennomgang viser imidlertid at den er av så lav kvalitet at den ikke kan brukes til å fastslå «skyld ut over enhver rimelig tvil», slik straffeloven er formulert i de fleste demokratiske rettsstater.
I 1971 publiserte den britiske nevrokirurgen Norman Guthkelch en teori om at kraftig risting kunne gi intrakraniale blødninger utenpå hjernen, selv uten ytre vold mot hodet. Denne teorien var basert på observasjoner hos bare to spebarn som hadde slike intrakraniale blødninger uten tegn til vold.
Etter denne publikasjonen ble stadig flere spebarn diagnostisert som «shaken baby» på grunn av likheten med Guthkelchs to spebarn, uten at noen hadde observert risting eller tegn til vold mot hodet.
Massiv filleristingslitteratur
Deretter bygget det seg opp en massiv filleristingslitteratur. Denne er blitt og blir fortsatt brukt som basis for sakkyndigerklæringer, som fastslår at filleristing har funnet sted, fortsatt uten at noen har sett ristingen. Hvordan kan det skje?
Antagelsen er basert på et sirkelresonnement: Fordi spebarn med slike intrakraniale blodvæskeansamlinger passer med Guthkelchs teori, blir de av barnevernsteam over hele verden diagnostisert som filleristet og lagt til den eksisterende datamengden. Det blir senere brukt som bevis på diagnostikkens nøyaktighet.
På slutten av livet var Guthkelch fortvilet over hvordan hans teori ble misbrukt, slik at uskyldige ble idømt straff og fratatt sine spebarn.Volume 0%00:0102:04
Tragedien «triaden»
I fravær av sikre bevis på mishandling, altså at noen faktisk har sett handlingen, baserer diagnosen filleristing seg på en kombinasjon av tre medisinske funn – den såkalte triaden: Blodansamlinger utenpå hjernen, blødninger i øyebunnen og røntgenologiske eller andre tegn til hjerneskade. Disse funnene er i tiår blitt brukt nærmest som sikre bevis i norsk rett på at spebarnet må ha blitt filleristet, selv om ingen har sett handlingen.
Skal «triaden» ha en slik rettslig beviskraft, må artiklene som påstår en sikker årsakssammenheng mellom «triaden» og risting være av så god vitenskapelig kvalitet at det ikke kan reises tvil om beviskraften. Problemet med «triaden» er at de medisinske funnene også finnes ved andre tilstander, tilstander som overhodet ikke har med mishandling å gjøre.Foreldrene ble anklaget for å ha filleristet «Tobias» (1) og trodde de aldri skulle få ham tilbake. Så begynte en pensjonert overlege å stille spørsmål.
Foreldre blir mistenkeliggjort
En offentlig svensk utredning fra 2016 (SBU-rapport 255/2016) baserte seg på gjennomgang av alle publiserte artikler om filleristing.
En komité bestående av svenske professorer og spesialister innen rettsmedisin, barnesykdommer, røntgendiagnostikk, medisinsk metodelære og etikk, konkluderte med at nesten alle disse artiklene baserte seg på sirkelbevisføring. De skriver at det er begrenset kunnskapsgrunnlag for at «triaden» i det hele tatt kan knyttes til voldsom risting, og at det erutilstrekkelig vitenskapelig grunnlag for å bruke «triadens» funn som bevis for at traumatisk risting har funnet sted.

Hvordan man bestemmer at et spebarn er filleristet, er ikke et medisinsk diagnostisk problem, det et samfunnsproblem, mener kronikkforfatterne. ILLUSTRASJONSFOTO: Standard store88 / Shutterstock / NTB scanpix
I tillegg til «triaden» legger medisinsk sakkyndige i slike rettssaker vekt på manglende troverdighet hos den som var alene med barnet da det plutselig ble dårlig. De sakkyndige har oftest som utgangspunkt at «triaden» bare kan skyldes filleristing.
Dersom foreldrene ikke kan gi en akseptabel forklaring på de medisinske funnene i form av en plausibel traumesykehistorie, er dét nok til å styrke mistanken eller gjøre filleristingsdiagnosen høyst sannsynlig. Og foreldrene kan jo nesten aldri gi en slik forklaring som de sakkyndige anser som «akseptabel», fordi barnets tilstand ikke skyldes et traume, men andre medisinske årsaker.Flere barn dør av mishandling enn i trafikkulykker
Ikke holdbar vitenskap
SBU-rapporten har ført til at så å si alle svenske rettsmedisinere i Sverige ikke lenger bruker «triaden» som bevis. Norske sakkyndige legger fortsatt avgjørende vekt på den i sine erklæringer.
Knut Wester har startet en faglig debatt i Tidsskrift for Den norske legeforening. Det lille antall sakkyndige som går igjen i nesten alle slike saker i Norge og alle er av samme mening, er utfordret til å komme med vitenskapelig holdbar dokumentasjon på at filleristingsdiagnosen kan stilles på basis av «triaden». De svarer riktignok at «funn av den såkalte triaden er i seg selv ikke tilstrekkelig som bevis i en straffesak». Vår erfaring er derimot at praksis viser noe annet i begge våre land.
Faktisk er det slik at bare ett funn – blod utenpå hjernen eller i øyenbunnen – er tilstrekkelig for å stille en så ødeleggende diagnose. De viser også til en konsensusartikkel som det viktigste grunnlag for sitt syn. Men heller ikke konsensus baserer seg på holdbar vitenskap.Blødninger, brudd, sår. Hvert år kommer 10–15 barn til norske sykehus med skader som kan gi mistanke om mishandling
Familier går i oppløsning
Konsensus befinner seg nederst på en rangering av medisinske bevis («evidens»). Det er en prosess for å bli enige om hva som er den beste måten å håndtere et medisinsk problem på når det ikke finnes holdbare bevis. I nødsfall kan det være bedre enn ingenting, men hvordan man bestemmer at et spebarn er filleristet, er ikke et medisinsk diagnostisk problem, det et samfunnsproblem.
Slutninger på feil grunnlag fører til at foreldre blir idømt lange fengselsstraffer, barn blir tatt fra foreldre og familier går i oppløsning.
Svenske og norske rettsmedisinere har totalt forskjellig syn på «triadens beviskraft». Begge kan ikke ha rett samtidig. I en slik uklar situasjon må man spørre seg om «skyld virkelig kan bevises utover enhver rimelig tvil» på grunnlag av «triadens» medisinske funn.
ACTA PÆDIATRICA Nurturing the child
Insufficient evidence for ‘shaken baby syndrome’ – a systematic review
Review Article Free Access
Niels LynøeGöran ElinderBoubou HallbergMåns RosénPia SundgrenAnders ErikssonFirst published: 27 January 2017 https://doi.org/10.1111/apa.13760 Cited by: 43
Abstract
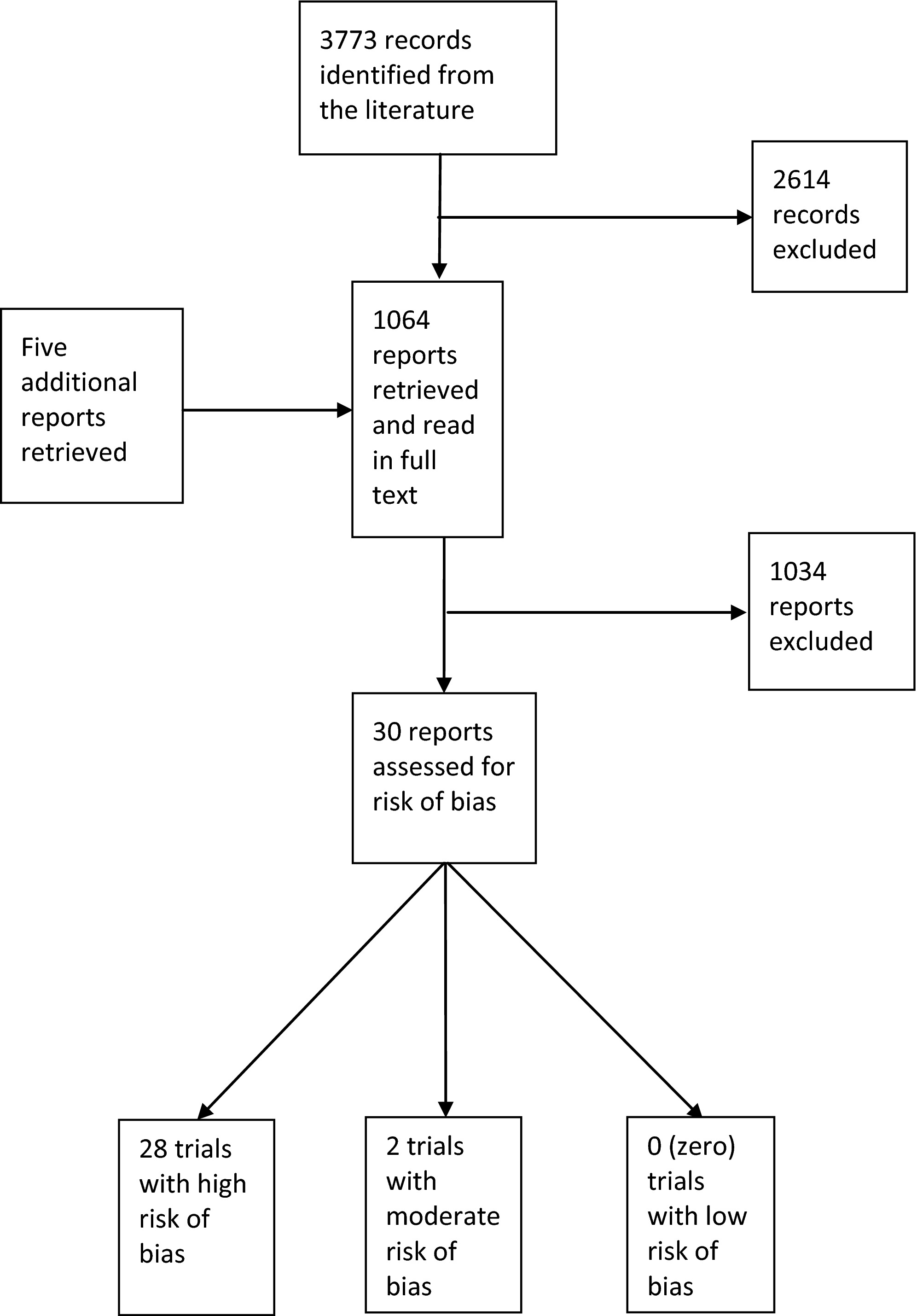
Shaken baby syndrome has typically been associated with findings of subdural haematoma, retinal haemorrhages and encephalopathy, which are referred to as the triad. During the last decade, however, the certainty with which the triad can indicate that an infant has been violently shaken has been increasingly questioned. The aim of this study was to determine the diagnostic accuracy of the triad in detecting that an infant had been shaken. The literature search was performed using PubMed, Embase and the Cochrane Library up to October 15, 2015. Relevant publications were assessed for the risk of bias using the QUADAS tool and were classified as having a low, moderate or high risk of bias according to predefined criteria. The reference standards were confessions or witnessed cases of shaking or accidents. The search generated 3773 abstracts, 1064 were assessed as possibly relevant and read as full texts, and 30 studies were ultimately included. Of these, 28 were assessed as having a high risk of bias, which was associated with methodological shortcomings as well as circular reasoning when classifying shaken baby cases and controls. The two studies with a moderate risk of bias used confessions and convictions when classifying shaken baby cases, but their different designs made a meta‐analysis impossible. None of the studies had a low risk of bias.
Conclusion: The systematic review indicates that there is insufficient scientific evidence on which to assess the diagnostic accuracy of the triad in identifying traumatic shaking (very low‐quality evidence). It was also demonstrated that there is limited scientific evidence that the triad and therefore its components can be associated with traumatic shaking (low‐quality evidence).
Key notes
- Shaken baby syndrome has typically been associated with findings of subdural haematoma, retinal haemorrhages and encephalopathy.
- However, the diagnostic accuracy of this triad in detecting that an infant has been shaken has been questioned.
- This systematic review indicates that there is insufficient scientific evidence on which to assess the diagnostic accuracy of the triad in identifying traumatic shaking (very low‐quality evidence).
Introduction
Rationale
The effects of abusively shaking an infant were first suggested by the paediatric neurosurgeon Norman Guthkelch in 1971. Based on a few cases, he introduced the hypothesis that shaking a baby backwards and forwards in a whiplash‐like manner might cause subdural haematoma and eventually other symptoms and signs, namely, retinal haemorrhages and encephalopathy, referred to as the triad 1, 2. These symptoms and signs could occur without visible signs of impact to the head and were associated with isolated violent shaking. An inverse version of the hypothesis was also eventually derived: if the triad was identified and no other ‘acceptable’ explanation was provided, the infant had been violently shaken 2.
During the last 40 or so years, a number of studies have been conducted on ‘shaken baby syndrome’ (SBS), which is currently a subset of more general labels such as abusive head trauma, nonaccidental head injury and similar terms (2, Box 1). It has been maintained by paediatricians and child protection teams (CPTs) that there is a scientifically robust body of knowledge supporting the general assumption that when the triad is observed, the infant has been violently shaken 3, 4. The criteria used to identify shaken baby cases 5 have also been used in criminal trials in order to prosecute and convict suspected perpetrators with the help of expert testimony. If the criteria are not reliable, however, this might result in either underdiagnosis or overdiagnosis, and the classification of shaken baby cases in scientific studies might be mistaken. Underdiagnosis is linked to an increased risk that the infant is not protected sufficiently as he or she is not separated from the perpetrator, while overdiagnosis might carry an increased risk of unjustly separating a family and prosecuting and convicting an innocent parent or guardian. Hence, robust and evidence‐based knowledge about the effects of shaking an infant has important medical and societal consequences for the concerned infant, the family, the general public’s trust in the medicolegal system and science in general.
Box 1. Explanations of the terminology used in the present text.
The term ‘shaken baby syndrome’ (SBS) signifies a constellation of symptoms and signs, viz. subdural haematoma, retinal haemorrhages and encephalopathy, often referred to as ‘the triad’ as caused by violent shaking.
The present review demonstrates that there is insufficient scientific evidence to support claims that the triad indicates that an infant has been violently shaken (very low‐qualityevidence), and that there is limited scientific evidence to support the assumption that shaking an infant can cause the triad (low‐quality evidence). The term ‘SBS’ is thus not justified, as it includes both the medical findings and the alleged, but scientifically unproven, injurious mechanism – and even the intent behind this mechanism. The same applies to a number of other ill‐defined terms used in the literature, for example ‘abusive head trauma’ (AHT), ‘nonaccidental head injury’ (NAHI), ‘inflicted head injury’ (IHI) or ‘NAHT’, which can symbolize two completely opposite meanings, viz. ‘nonabusive head trauma’ and ‘nonaccidental head trauma’.
Hence, the authors have in this study avoided the acronyms above and chosen to differ distinctly between the injurious mechanism (‘traumatic shaking’) and the medical findings(the symptoms and signs, ‘the triad’). Intent is not, for obvious reasons, for the medical community to decide.
Over the last decade, questions about the validity of the allegedly strong link between the triad and traumatic shaking have successively increased 6–8. Norman Guthkelch, and others, has questioned the manner in which his own original hypothesis, as well as the subsequent inverse version of the hypothesis, became dogma and has claimed that the evidence on which the hypothesis was based is poor 9.
Objectives
The main objective of this systematic review was to determine the diagnostic accuracy of the triad in detecting that an infant had been violently shaken.
Methods
Protocol and registration
This systematic review was conducted at the Swedish Agency for Health Technology Assessment and Assessment of Social Services and published in Swedish in October 2016 as a report at www.sbu.se/2016. The agency used a peer‐reviewed protocol, including prespecified objectives in accordance with standards in health and technology assessments. For the used terms traumatic shaking and SBS, see Box 1.
As this study is based on a literature review, no patients or participants were involved.
Eligibility criteria
The eligibility criteria were as follows. The population was infants of 12 month or under 12 months of age, and the index test was the presence of the triad in suspected traumatic shaking. The gold standard reference test was either that someone had confessed to shaking a baby, or other documented trauma, and the outcome was diagnostic accuracy.
Case–control and cohort studies with fewer than 10 individuals were excluded to minimise the risk of selection bias. For possible differential diagnoses, also studies of single cases could challenge the hypothesis that the triad always is caused by traumatic shaking. Studies of differential diagnoses were not assessed regarding quality and were consequently not a basis for the results. Studies including children older than 12 months of age, or with signs of impact to the head, were included only if a subgroup of 12 month or under 12 months of age, and/or a subset of isolated shaking, was identified.
Information sources and search terms
The electronic literature search was performed by an information specialist and included PubMed, Embase and the Cochrane Library up to October 15, 2015. A complementary manual search was conducted among the references in literature reviews and publications not identified in the main search. Studies published in English, German, French, Swedish, Norwegian and Danish were included. Grey literature, such as conference abstracts or dissertations, was not included.
The search terms included, but were not restricted to, infant, subdural haematoma, retinal haemorrhage, cerebral oedema, encephalopathy, accidental and nonaccidental injury, shaken baby and SBS 2.
Study selection
Six reviewers were engaged in the process and were split into three groups of two reviewers. They independently screened the titles and abstracts identified through the search strategy. The full texts of all studies of potential relevance according to the inclusion criteria were obtained, and each group of two reviewers assessed one‐third of them for inclusion. Any disagreement was resolved by discussion until a consensus was reached.
Data collection process and data items
Information concerning the study design, population and results was extracted from the included papers with a low or moderate risk of bias.
Risk of bias in individual studies
Two reviewers independently assessed the risk of bias in individual studies using a modified version of the QUADAS tool 10. Each study was rated as having a low, moderate or high risk of bias. The judgement of the risk of bias focused on the risk of systematic errors due to methodological flaws, including circular reasoning in the classification of shaken baby cases and controls. Systematic literature reviews were assessed using the AMSTAR instrument 11.
Studies were assessed as having a low risk of bias when the study cases, namely shaken babies, were unequivocally confirmed as having been violently shaken and when the shaking preceded the symptoms associated with the triad, for example by a video recording or independent witness information. Furthermore, the control cases needed to have been age‐matched and unequivocally subjected to other defined types of trauma.
Studies were assessed as having a moderate risk of bias when the shaken baby study cases were identified as the result of a detailed confession by the suspected perpetrator and/or when there were shortcomings regarding controls, for example no age match or even a lack of controls. Each individual study underwent an overall assessment with regard to the significance of such shortcomings.
Studies were assessed as having a high risk of bias when additional deficiencies were present, and it was judged that the results could not provide reliable information in response to the questions addressed in this systematic review, for example insufficient definition of the study cases and circular reasoning.
Risk of circular reasoning
In many studies, the authors referred to a child protection team (CPT) when classifying shaken baby cases and controls. The CPT and concerned paediatricians often took for granted that if the triad was present, and no other acceptable explanations were provided, that the infant had been violently shaken 12. The criteria for what was considered an ‘acceptable’ explanation had also been developed, and if these criteria were not fulfilled, a case was classified, by default, as a shaken baby case (Table 1). The research question for this study concerned the certainty of the conclusion that an infant had been violently shaken when the triad was observed. But if what was going to be examined had already been taken for granted by those who were classifying the cases, the result was judged to have been based on circular reasoning. To avoid circular reasoning, only studies in which someone had confessed to shaking the child were included.Table 1. The child protection teams’ and the scientists’ criteria for cases classified as shaken babies and controls
| Shaken babies | Controls | |
|---|---|---|
| Lack of explanation | Yes | |
| Accidental fall <1 m | Yes | |
| Accidental fall >1 m | Yes | |
| Not witnessed accidents | Yes | Yes |
| Witnessed accidental fall | Yes | |
| Witnessed shaking | Yes | |
| Confessed shaking + details | Yes | |
| False confession + details | Yes | |
| Confessed milder resuscitation shaking | Yes | |
| Cases in which someone is convicted | Yes | |
| Cases in which caretakers change story | Yes |
Method of analysis
As sensitivity and specificity were not presented, or could not be calculated from the included studies, it was not possible to conduct a meta‐analysis.
Results
Study selection
The literature search generated 3773 records, of which 1064 were original papers of potential relevance and were read as full texts. Of these, 1034 did not fulfil the inclusion criteria and were subsequently excluded, resulting in 30 included papers. Of these, 28 were assessed as having a high risk of bias 13–40, two as having a moderate risk 41, 42 and none as having a low risk (Fig. 1).
The assessed systematic literature reviews were all ranked as being of low quality 43–49.
Study characteristics and risk of bias within studies
The strength of the two included studies with a moderate risk of bias 41, 42 – one retrospective and one prospective – was the fact that their study groups were based on confessions. One study provided detailed information about the shaking event in 14 of 29 cases 41, while the control group in the other study entailed witnessed accidents in public areas 42. One methodological weakness of both the included studies was the risk of false confessions, but there were also other methodological flaws.
Results of individual studies
In the retrospective case–control study 41, the group of confessed shaking cases was compared to a group containing people who were suspected of, but denied, having shaking the infant. In the confessed shaking group, 13 of the 29 cases were allegedly injured through isolated shaking, and detailed information about the shaking event was provided in 14 of the 29 cases. A similar specification was not provided in the denial group, which comprised 82 cases. The authors found no statistically significant differences between the cases in the two groups, with regard to their age, sex, mortality, symptoms, etc.
In the prospective study 42, the authors compared a group of infants in which someone had confessed to and/or been convicted of having shaken the baby (n = 45) with a group in which the infants had been exposed to an accident that was witnessed in a public area (n = 39). The authors stated that ‘Information on the confessions was obtained by a forensic paediatrician from judicial sources during expertise or after the judicial hearings were made public’ 42. No detailed information was provided regarding what had been confessed or under what circumstances the confessions had been obtained. The authors used a triad that comprised subdural haematoma, diffuse retinal haemorrhages and an absence of scalp swelling. For the applied triad, the authors reported a sensitivity of 0.244, a specificity and positive predictive value of 1.0 and a negative predictive value of 0.534.
Different conditions or events that might have caused the triad or its components included accidental trauma, such as a fall or motor vehicle accident, sequelae of normal delivery, prematurity, macrocephaly and external hydrocephalus, coagulopathies, infections, metabolic diseases, leukaemia, immunological conditions, vascular malformations in the brain and asphyxia 2.
Discussion
Summary and evidence
The main finding was that 28 of the 30 included studies were assessed as having a high risk of bias, while two had a moderate risk and none had a low risk. There were two main indications of a high risk of bias: methodological flaws and circular reasoning when classifying shaken baby cases and controls. Two conclusions were drawn. The first was that there is insufficient scientific evidence on which to assess the diagnostic accuracy of the triad in identifying traumatic shaking [very low‐quality evidence according to GRADE measure 50]. The second was that there is limited scientific evidence that the triad and therefore its components can be associated with traumatic shaking [low‐quality evidence according to GRADE 50].
Limitations of the studies identified
The included studies were observational, and many of them used comparison groups and were performed as retrospective case–control studies extracted from medical records or registers. Some studies were designed as prospective cohort studies. Apart from the usual methodological bias issues associated with retrospective case–control studies, other issues were also observed. In most studies, the average age of the control group was significantly higher than that of the shaken baby group, particularly in accidental falls 51. Furthermore, the radiological and ophthalmological examinations were rarely blinded, and, when they were, a poor or moderate inter‐rater agreement was reported 52.
The criteria for classifying study cases and controls varied. Sometimes the composition of the comparison group was explicitly presented, whereas sometimes there was simply a deferral to the judgement of a CPT. Sometimes the criteria for shaken baby cases were related to controversies concerning the height of a fall. If the fall was below a certain height, for example 1 m, the case was classified as a shaken baby, but if it was above 1 m, it was classified as a control (see Table 1). Such classifications were applied, despite the fact that several studies have shown that a minor fall could have caused the triad, particularly in cases of increased head circumference due to macrocephaly – benign enlargement of the subarachnoid space in infancy 53–56 – or long‐term sequelae of a chronic subdural haematoma after an uncomplicated vaginal delivery 20, 57–59. Such classification criteria resulted in uncertainty as to whether the groups of shaken babies also included accidental injury cases and whether the control groups also contained shaken babies.
The other main reason for the low quality was the issue of circular reasoning linked to the classification criteria. As illustrated in Table 1, in many cases, the applied criteria focused more on the suspect’s trustworthiness than on scientifically based criteria.
The two studies of moderate quality
The two studies of moderate quality included samples in which a person had confessed to and/or been convicted of having shaken an infant 41, 42.
In one study 41, those who had confessed provided detailed information about the shaking event in approximately half of the cases. No significant difference was found between the two groups of those who had confessed and those who had not. Three interpretations seem plausible: either the group who confessed to a shaking event included false confessions, or the group who denied a shaking event actually included shaken babies, or both. The circumstances under which a confession was obtained might have involved false confessions, because of police pressure, or be the result of plea‐bargaining procedures, which also entail an increased risk of false confession 60, 61. It is not known whether police‐induced confessions or plea‐bargaining procedures were applied in any of the two studies.
In the other study of moderate quality 42, the authors compared a group in which someone had confessed to having shaken an infant to a control group where an accidental trauma had been witnessed in a public area. However, as the authors used a different triad – with encephalopathy replaced by the absence of scalp swelling – it was not possible to calculate specificity and positive predictive value for the traditional triad. The shaking group was compared to a group with accidental injuries, all of which were very likely to have had signs of external impact to the head or skull. Accordingly, it is no surprise that the authors obtained a specificity and predictive value of 100%. Furthermore, as the authors used different ratings of retinal haemorrhages, the modified triad was even more complicated. Moreover, the nature of the confessions was not reported.
Due to the low quality of the reviewed studies, the incidence and prevalence of SBS remain unknown.
Other conditions and events that could have caused the triad
The literature search identified a large range of diseases and events that were associated with the triad or its components. The various diagnoses and events were more or less common, and the various conditions were more or less controversial, such as rebleeding after a minor fall in a child with an enlarged head circumference 20, 53–59. Another controversial issue was whether normal vaginal delivery was associated with subdural haematoma and retinal haemorrhages in around 30% of newborn infants 62–65; the incidence was reported to be higher in assisted deliveries and significantly lower in scheduled Caesarean deliveries. As far as we know, these phenomena were clinically asymptomatic and the haematomas and haemorrhages resorbed within months. In a few cases, however, the subdural haematoma might have developed into a chronic subdural haematoma or hygroma, which might have resulted in symptomatic rebleeding, either spontaneously or after a minor trauma 20, 57–59. These possibilities complicate the picture when an infant suddenly presents with symptoms such as apnoea and its parent or guardian is unable to provide an ‘acceptable’ explanation for these symptoms.
Ethical considerations
All children must be protected from abuse, and it is also important that families are not unnecessarily separated and that innocent parents or guardians are not convicted. From the clinical perspective of a CPT, it might be more important to protect the infant from abuse than to prevent the conviction of an innocent parent or guardian. But it is a problem if scientists base their classifications on the preferences of a CPT. To date, such teams have provided scientists with biased classification criteria, resulting in biased studies that by default support already established but biased evidence. Epidemiologists found that the incidence of homicide among infants from 1980 to 2005 sharply increased from a stable incidence during the period 1940–1979 66. The authors suggested that the classification of homicides and accidental deaths in recent decades had been influenced by ethical considerations rather than by scientifically based consideration.
To obtain valid knowledge, future research must avoid circular reasoning when classifying shaken baby cases and controls (Table 2).Table 2. Recommendations and cautions when conducting future research within the field of shaken baby
| Prospective cohort and case–control studies |
|---|
| When classifying shaken baby cases, demand information about the following: |
| police interrogation methods (risk of false confession)the presence of plea bargain (risk of false confession)role of child protection teamwhat the suspect has actually confessedwhether and how differential diagnoses were excluded |
| When classifying controls, demand information about the following: |
| witnessed events in a public areaage matchingrole of child protection team |
| Avoid circular reasoning when classifying cases and controls! |
| Other requested studies |
| Screening of newborns for subdural haematoma and retinal haemorrhagesNatural course of subdural haematoma and retinal haemorrhages among newbornsVulnerability of infants with macrocephalyBlinding of observations of subdural haematoma and retinal haemorrhagesPhysiological mechanisms of shaking |
Conclusion
This review showed there is insufficient scientific evidence on which to assess the diagnostic accuracy of the triad in identifying traumatic shaking (very low‐quality evidence). Furthermore, there is limited scientific evidence that the triad and therefore its components can be associated with traumatic shaking (low‐quality evidence).
As valid knowledge is necessary to determine whether or not an infant has been violently shaken, future research requires that circular reasoning be avoided when classifying shaken baby cases and controls.
Acknowledgements
We gratefully acknowledge the administrative and secretarial support provided by Anna Attergren Granath, Irene Edebert, Frida Mowafi and the literature searches conducted by documentation specialist Hanna Olofsson.
Finance
This review was funded by, and conducted at, the Swedish Agency for Health Technology Assessment and Assessment of Social Services.
Conflicts of interest
None of the authors have any conflict of interests to declare.